Feeding skill, Appetite and Feeding Behaviours of Infants and Young Children and Their Impact on Growth and Psychosocial Development
Maria Ramsay, PhD
McGill University, Canada
, 2nd rev. ed.
Introduction
Feeding, like other sensorimotor skills, is a developmental skill that matures during the first two years of life. It is a highly complex sensorimotor process with developmental stages based on neurological maturation and experiential learning.1 However, feeding, unlike other sensori-motor skills, is heavily reliant on internal incentive or motivation to initiate ingestion, and is essential for survival of the newborn. Thus, the act of feeding is highly charged emotionally for the mother, whose primary responsibility, as viewed by the family, society and culture around her, is to ensure the early growth and well being of her child. Therefore, from the very beginning the mother-infant feeding relationship is influenced by physiologic as well as interactional forces at multiple levels.2
Subject
When feeding skills are intact and appetite is robust, feeding times, and later on, mealtimes are a source of pleasant socialisation resulting in adequate nutrient intake and good growth. Demanding food at regular intervals, sucking, eating and drinking with good rhythm, trying new food tastes or textures, and expressing satisfaction at the end of feeding are all considered good feeding behaviours by family and society. These pro-feeding behaviours invite praise and positive feeding interactions and thus reinforce the feeling of self-mastery in the young child and promote continued food acceptance and independent feeding behaviours.
However, when feeding skills are impaired (e.g.: poor oral-motor skills, taste and texture sensitivities) and or poor appetite (inadequate hunger), they manifest themselves in problematic feeding behaviours such as not signalling hunger, sucking or eating excessively slowly, gagging, and not bringing food to the mouth.3-7 In addition, associative conditioning to painful gastrointestinal cues is particularly powerful in young infants and this conditioning often manifests itself in problematic feeding behaviours.8,9 Temperamental characteristics and regulatory capacities of the infant may further modulate feeding behaviours.10,11 Maternal attempts at increasing her infant’s nutrient intake by feeding more frequently or longer duration tend to result in stressful feeding experiences for both.12 While these efforts may work well initially for maintaining good weight gain, they tend to become ineffective and maladjusted mealtime interactions and behavioural mismanagement prevail.2,13-15 Maternal and family characteristics and societal expectations about the size of the young child and the type of food eaten further influence an already stressful feeding relationship.16,17
Problems
Feeding difficulties are one of the most common developmental disturbances in otherwise healthy infants and young children, often resulting in poor growth. Although an estimated 25%- 50% of children experience transient feeding problems under two years of age,18,19 most feeding issues resolve by the end of early childhood. However, an estimated 3-10% of children present with more severe forms of feeding problems which put children at risk for impaired growth, chronic illnesses and behavioural developmental problems.20 As well, a large percentage of children with special needs, children with developmental disabilities and children born prematurely have severe and chronic feeding problems where families need support in resolving the feeding issues.21-23 At the clinical level, the mother (and her paediatrician) is often not aware of the underlying reasons for problematic feeding behaviours. Thus, the mother’s reactions to a poor feeder may be exposed to covert or overt family criticism, which often lead to internal doubt about her own ability to nurture.4 At the policy level, there is a lack of education of professionals and young parents about feeding as a highly complex developmental skill, motivated by hunger and conditioned by parental reactions. Furthermore, professionals are still not trained to recognize that when either feeding skills or motivation or both are impaired, problematic feeding behaviours, stressed mealtime interactions and family conflicts are likely to result.
Research Context
Earlier cross-sectional clinical studies examined the relationship between feeding difficulties and attachment, maternal characteristics, family dynamics24 and feeding practices.24-30 These studies were conducted prospectively, that is, after the children were diagnosed with poor growth. Several observational studies focused on feeding interactions and problematic feeding behaviours.31,32 The development of feeding and patterns of food acceptance have been studied by numerous psychologists.33-36 More recently, few researchers started to focus on possible pathophysiology (heart rate variability, hormonal balance) of poor growth and problematic feeding behaviours.37-39 Other studies were conducted in the context of primarily behavioural interventions for problematic feeding behaviours in medically ill and very premature infants.40-43
Key Research Questions
The extensive research in the area of feeding problems and poor growth can be divided along the following three research questions:
- How do maternal (family) characteristics (cognitive abilities, personality disorders, psychological status and early attachment history) influence feeding behaviours and growth?
- How do infant characteristics (feeding skills, appetite, temperament and other physiological characteristics) influence feeding behaviours, mealtime interactions and growth?
- How effective are behavioural and other forms of intervention for severe problematic feeding behaviours in medically ill infants?
Recent Research Results
Only questions 2 and 3 will be summarised here. With a focus on infant characteristics, studies have shown that feeding problems often co-occur with sleeping and behavioural disturbances (irritability, poor self-calming and intolerance to change), suggesting that these are symptoms of a common underlying constitutional “regulatory disorder” in infants and young children.44,45 In a large whole-population survey of children’s growth and development, a significant portion (36%) of the 47 children identified with failure to thrive at one year of age were found to have oral motor difficulties, suggesting that these children were biologically more vulnerable to poor eating from birth.46 Another study showed that young infants with gastroesophageal reflux were significantly more likely to have delay in their feeding skills and readiness behaviour for solids than controls.47 In a prospective study of a group of healthy term infants (n=330), infants with inefficient sucking, as measured by tracings on a polygraph, at one week and two months were significantly more likely to have mothers with greater effort at feeding than infants with efficient sucking.14
A number of studies have shown that children under 3 to 4 years of age eat primarily in response to appetite or hunger cues, whereas older children’s eating are influenced by a variety of environmental (extra food available) and social factors.48,49 As well, children with poor growth were observed to refuse offered food more often and fed themselves significantly less often than controls.50 In terms of the third question, the literature reflects the reality that presently we are better at identifying factors contributing to feeding problems at any level of severity than treating them.28,51,52 Treating feeding problems at the primary or secondary level, while desirable, is not always available for parents.53 Treating feeding disorders associated with severe medical illnesses, developmental disabilities and gavage feedings requires the collaboration of multidisciplinary teams for successful outcome.54-59 Lastly, studies have shown that appetite stimulating medications result in good weight gain, and thus making intervention more efficacious.60-62
Conclusions
Understanding feeding behaviours requires the knowledge of feeding as a developmental skill that matures over time and is reliant on hunger (appetite) cues and experiential learning. Whereas feeding skills are well established by two years of age, hunger cues shift from primarily internal to external (family, school and societal) control only by 4-5 years. Thus, although initially problematic feeding behaviours tend to be reactions to internal cues, these behaviours can become conditioned to external (coaxing parents) and societal cues. Medical illnesses, prematurity and developmental disorders further interfere with the development of normal feeding behaviours.
In order to help identify feeding problem, a number of feeding scales have been devised,63-65 but rarely used for assessment or treatment outcome. Yet, early behavioural intervention can play an important role in normalizing feeding behaviours and mealtime interactions, which in turn help promote independence and other self-help skills in the child. Most recently, an easy and short screening tool was developed for detecting problematic feeding behaviours in primary care offices, allowing early referral to appropriate feeding clinics.66
An example of a Feeding Scale, which takes only 5 minutes to fill and may be filled by a pediatrician or nurse or other professionals, given that they possess the necessary information about infant/child feeding, or know where to refer the child with feeding problems.
Implications for Policy and Services
The major findings from this updated summary continue to be that the physiological make up of the infant, medical illnesses, developmental disabilities and parental responses all play an important role in the dynamic relationship in which problematic feeding behaviours develop. This finding has several implications for policy and services in hospitals where premature infants and infants with medical needs grow poorly, requiring enteral feedings. Thus, intervention with staff specialized in feeding disorders, usually occupational or speech therapists, help initiate oral feedings. As well, doctors or pediatricians following infants and young children need continued education in possible causes of poor growth in otherwise healthy infants.
- At the primary care level, the use of easy to administer feeding scales for earlier detection and thus, treatment of feeding problems should continue to be advocated. (See an example of the Feeding Scale below).
- The continuation of mandated multidisciplinary feeding clinics addressing feeding disorders in hospital settings. These feeding programs need to be easily accessible to parents, where effective behavioural intervention and preventive strategies may be implemented in the early stages of reported difficult feeding behaviours.
- The training of experts in the field of feeding disorders, which should include training in the behavioural, developmental and interactional components of feeding, as well as understanding the physiological, as well as the medical components should be advocated.
The Pediatric Feeding Program' research at The Montreal Children's Hospital:
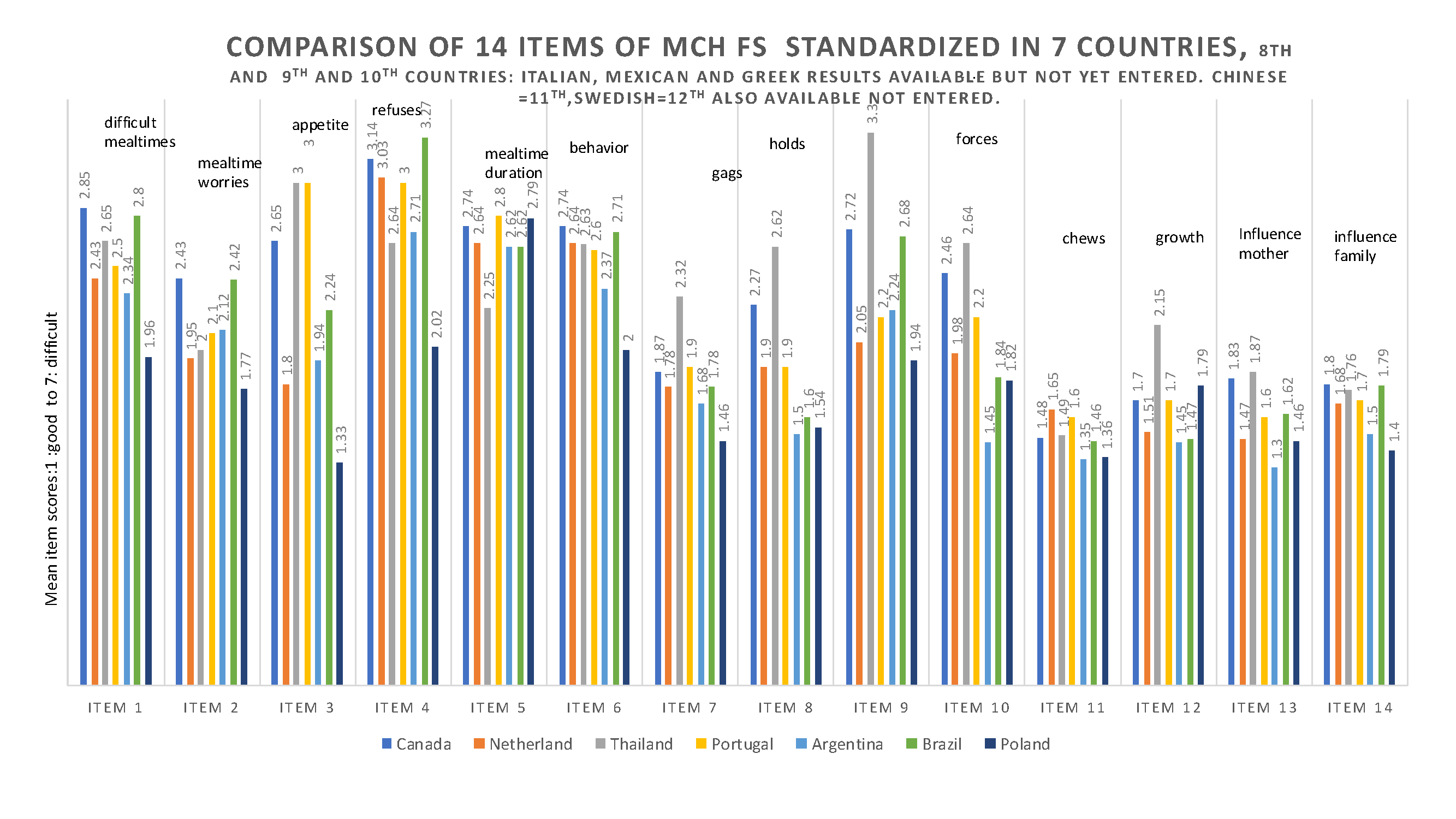
Feeding infants and young children can be challenging. Initially, the feeding scale was developed to have a common language with the mothers about feeding difficulties they experience with their children, and to assess the intervention. This scale (MCH-FS) has become known word-wide, and as of now, it has been translated and standardized on a healthy children population in Montreal and in several other countries. The author of this article has approved all translations by using back-translations before the translated version could be used in 8 languages. Depicted in the graphic below is only 7 as Canada used the results of the English and French languages combined.66-77 The scale was later translated and standardized in another four languages: Italian71, Mexican70,75 Turkish76 and Chinese77.
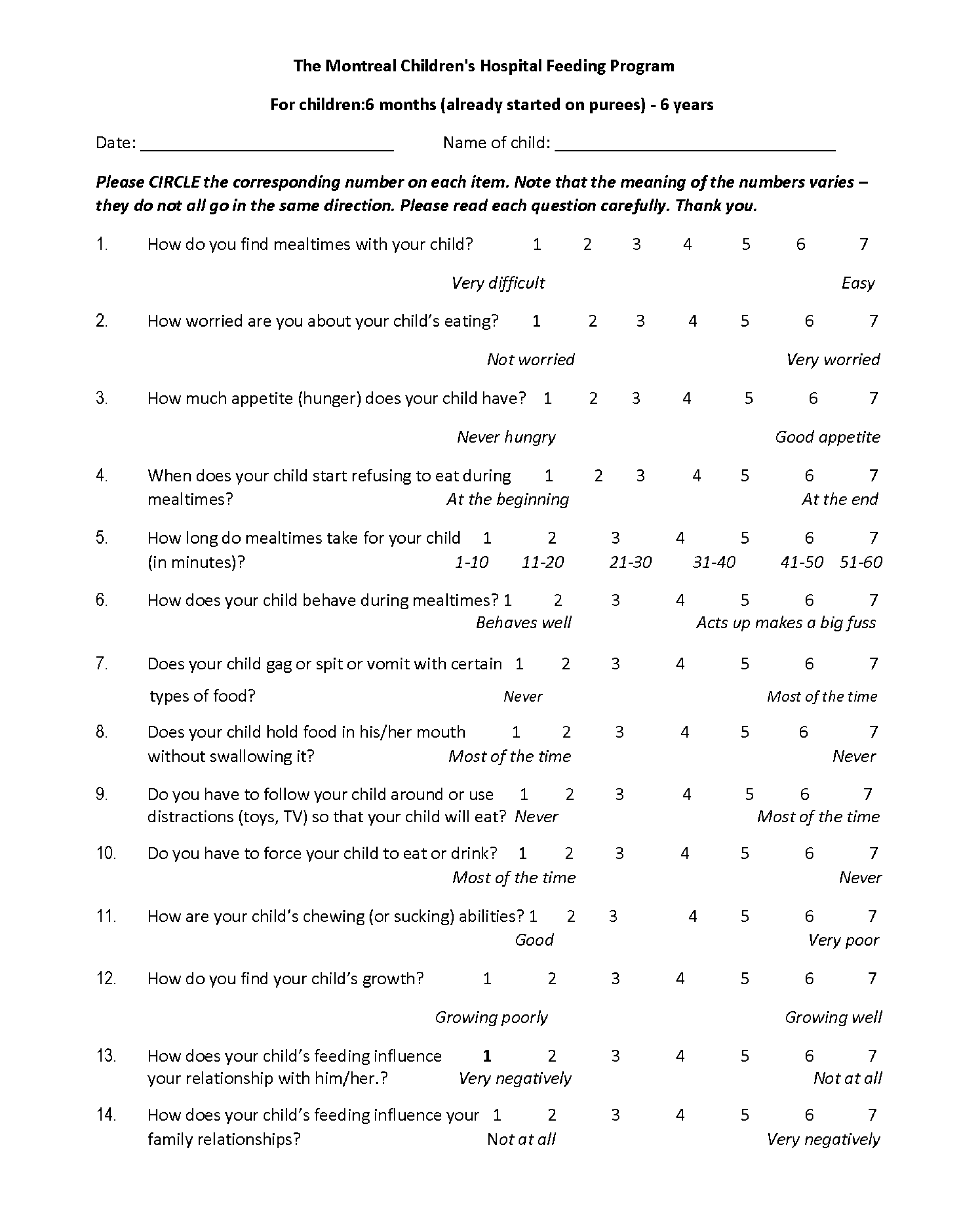
See the MCH-FS above: Of note is that other infant/child feeding scales do not take into consideration the variability of infant/child level of appetite, which influences maternal approach to feeding and the child's acceptance of food.66-77
References
- Stevenson RD, Allaire JH. The development of normal feeding and swallowing. Development and behavior: The very young child. Pediatric Clinics of North America. 1991;38(6):1439-1453.
- Ramsay M. Les problèmes alimentaires chez les bébés et les jeunes enfants : Une nouvelle perspective. PRISME. 1999;30:10-27.
- Milla PJ. Feeding, tasting and sucking. In: Walker WA, Durie P, Hamilton J, Walker-Smith J, Watkins J, eds. Pediatric gastrointestinal disease: pathophysiology, diagnosis, management. Philadelphia, PA: DC Decker; 1991:217- 223.
- Ramsay M. Feeding disorder and failure to thrive. Child and Adolescent Psychiatric Clinics of North America. 1995;4(3):605-616.
- Reau NR, Senturia YD, Lebailly SA, Christoffel KK. Infant and toddler feeding patterns and problems. Normative data and a new direction. Journal of Developmental and Behavioral Pediatrics. 1996;17(3):149-153.
- Jacobi C, Agras WS, Bryson S. Hammer LD. Behavioral validation, precursors and concomitants of picky eating in childhood. Journal of the American Academy of Child and Adolescent Psychiatry. 2003;42(1):76-84.
- Ramsay M, Gisel EG, Boutry M. Nonorganic failure to thrive: A growth failure secondary to feeding skills disorder. Developmental Medicine and Child Neurology. 1993;35(4):285-297.
- Davidson TL. Pavlovian occasion setting: a link between physiological change and appetitive behavior. Appetite. 2000;35(3):271-272.
- Hamilton AB, Zeltzer LK. Visceral pain in infants. Journal of Pediatrics. 1994;125(6 Pt 2):S95-102.
- Harris G, Blissett J, Johnson R. Food Refusal Associated with Illness. Child Psychology and Psychiatry Review. 2000;5(4):148-156.
- DeGangi GA, Porges SW, Sickel RZ, Greenspan SI. Four-year follow-up of a sample of regulatory disordered infants. Infant Mental Health Journal. 1993;14(4):330-343.
- Ferguson A, Blaymore Bier LA, Cucca J, Andereozzi L, Lester B. The quality of sucking in infants with colic. Infant Mental Health Journal. 1995;17(2):161-169.
- Ramsay M, Gisel EG. Neonatal sucking and maternal feeding practices. Developmental Medicine and Child Neurology.1996;38(1):34-47.
- Ramsay M, Gisel E, McCusker J, Bellevance F, Platt R. Infant sucking ability, nonorganic failure to thrive, maternal characteristics and feeding practices: A prospective cohort study. Developmental Medicine and Child Neurology. 2002;44(6):405-414.
- Budd KS, McGraw TE, Farbisz R, Murphy TB, Hawkins D, Heilman N, Werle M, Hochstadt NJ. Psychosocial concomitants of children's feeding disorders. Journal of Pediatric Psychology. 1992;17(1):81-94.
- Farrow C, Blissett J. Maternal cognitions, psychopathologic symptoms and infants temperament as predictors of early infant feeding problems: A longitudinal study. International Journal of Eating Disorders. 2006;39(2):128-134.
- Knaapila A, Tuorila H, Silventoinen K, Keskitalo K, Kallela M, Wessman M, Peltonen L, Cherkas LF, Spector TD, Perola M. Food neophobia shows heritable variation in humans. Physiology & Behavior. 2007;91(5):573-578.
- McDermott BM, Mamun AA, Najman JM, Williams GM, O'callaghan MJ, Bor W. Preschool children perceived by mothers as irregular eaters: Physical and psychosocial predictors of a birth cohort study. Journal of Developmental and Behavioral Pediatrics. 2008: 29(3):197-205.
- Carruth BR, Zeigler PJ, Gordon A, Barr SI. Prevalence of picky eaters among infants and toddlers and their caregivers’ decisions about offering a new food. Journal of the American Dietetic Association. 2004;104(1 Suppl 1):S57-S64.
- Corbett SS, Drewett RF. To what extent is failure to thrive in infancy is associated with poorer cognitive development. A review and meta-analysis. Journal of Child Psychology and Psychiatry, and Allied Disciplines. 2004;45(3):641-654.
- Lenscheid TR. Behavioral treatments for pediatric feeding disorders. Behavior Modification. 2006;30(1):6-23.
- SJ, Harris G, Blissett J. Tube feeding in infancy: Implications for the development of normal eating and drinking skills. Dysphagia. 2005;20(1):46-61.
- Cerro N, Zeunert S, Simmer KN, Daniels LA. Eating behaviour of children 1.5-3.5 years born preterm: Parents’ perceptions. Journal of Paediatrics and Child Health. 2002;38(1):72-78.
- Piwoz EG, Black RE, Lopez de Romana G, Creed de Kanashiro H, Brown KH. The relationship between infants’ preceding appetite, illness, and growth performance and mothers’ subsequent feeding practice decision. Social Science & Medicine. 1994;39(6): 851-860.
- Benoit D. Failure to thrive and feeding disorders. In: Zeanah CH Jr, ed. Handbook of infant mental health. New York, NY: Guilford Press; 1993:317-331.
- Galler JR, Harrison RH, Biggs MA, Ramsey F, Forde V. Maternal moods predict breastfeeding in Barbados. Journal of Developmental and Behavioral Pediatrics.1999;20(2):80-87.
- Polan HJ, Kaplan MD, Kessler DB, Schindledecker R, Mewmark M, Stern D, Ward MJ. Psychopathology in mothers of infants with failure to thrive. Infant Mental Health Journal. 1991;12(1):55-64.
- Ward MJ, Kessler DB, Altman SC. Infant attachment in children with failure to thrive. Infant Mental Health Journal. 1993;14(3):208-220.
- Lindberg L, Bohlin G, Hagekull B, Thurnström M. Early food refusal: Infant and family characteristics. Infant Mental Health Journal. 1994;15(3):262-277.
- Parkinson NK, Drewett RF. Feeding behaviour in the weaning period. Journal of Child Psychology and Psychiatry. 2001;42(7):971-978.
- Lindberg L, Bohlin G, Hagekull B. Interactions between mothers and infants showing food refusal. Infant Mental Health Journal. 1996;17(4):334-347.
- Stein A, Woolley H, Cooper SD, Fairburn CG. An observational study of mothers with eating disorders and their infants. Journal of Child Psychology and Psychiatry. 1994;35(5):733-748.
- Birch LL, Gunder L, Grimm-Thomas, Laong DG. Infants’ consumption of a new food enhances acceptance of similar foods. Appetite. 1998;30(3):283-295.
- Birch LL. Development of food acceptance patterns. Developmental Psychology. 1990;26(5):515-519.
- Beauchamp GK, Mennella JA. Flavor perception in human infants: Developmental and functional significance. Digestion. 2001;63 Suppl 1:1-6.
- Coulthard H, Harris G, Emmett P. Delayed introduction of lumpy foods to children during the complementary feeding period affects child’s food acceptance and feeding at 7 years of age. Maternal and Child Nutrition. 2009;5(1):75-85.
- Shaoul R, Kessel A, Toub, E, Lanir A, Glazer O, Jaffe M. Leptin and cytokines levels in children with failure to thrive. Journal of Pediatric Gastroenterology and Nutrition. 2003;37(4):487-491.
- Steward DK, Moser DK, Ryan-Wenger NA. Biobehavioral characteristics of infants with failure to thrive. Journal of Pediatric Nursing. 2001;16(3)162-171.
- Tannenbaum GS, Ramsay M, Martel C, Samia M, Zygmuntowicz C, Porporino M, Ghosh S. Elevated circulating acylated and total ghrelin concentrations along with reduced appetite scores in with failure to thrive. Pediatric Research. 2009;65(5):569-573.
- Babbitt RA, Hoch RA, Coe DA, Cataldo MF, Kelly KJ, Stackhouse C, Perman JA. Behavioral assessment and treatment of pediatric feeding disorders. Journal of Developmental and Behavioral Pediatrics. 1994;15(4):278-291.
- Burklow KA, Phelps AN, Schultz JR, McConnell, Rudolph C: Classifying complex pediatric feeding disorders. Journal of Pediatric Gastroenterology and Nutrition. 1998;27(2):143-147.
- Werle MA, Murphy TB, Budd KS. Treating chronic food refusal in young children: Home-based parent training. Journal of Applied Behavior Analysis. 1993;26(3):421-433.
- Burmucic K, Trabi T, Deutschmann A, Scheer PJ, Dunitz-Scheer M. Inpatient tube weaning in children with long-term feeding tube dependency: A retrospective analysis. Infant Mental Health Journal. 2010;31(6):664-681
- St.James-Roberts I, Plewis I. Individual differences, daily fluctuations, and developmental changes in amounts of infant waking, fussing, crying, feeding, and sleeping. Child Development. 1996;67(6):2527-2540.
- Wolke D, Gray P, Meyer R. Excessive infant crying: A controlled study of mothers helping mothers. Pediatrics. 1994;94(3):322-334.
- Reilly SM, Skuse DH, Wolke D, Stevenson J. Oral-motor dysfunction in children who fail to thrive: organic or non-organic. Developmental Medicine and Child Neurology. 1999;41(2):115-122.
- Mathisen B, Worrall L, Mase; J, Wall C, Shepherd RW. Feeding problems in infants with gastro-oesophageal reflux disease: a controlled study. Journal of Paediatrics and Child Health. 1999;35(2):163-169.
- Fisher JO, Birch LL. Eating in the absence of hunger and overweight in girls from 5 to 7 year of age. American Journal of Clinical Nutrition. 2000;76(1):226-231.
- Rolls BJ, Engell D, Birch LL. Serving portion size influences 5-year-old but not 3-year-old children’s food intakes. Journal of the American Dietetic Association. 2000;100(2):232-234.
- Drewett RF, Mambwe K-H, Wright C. Feeding behaviour in young children who fail to thrive. Appetite. 2003;40(1):55-60.
- Wright C, Birks E. Risk factors for failure to thrive: A population-based survey. Child: Care, Health and Development. 2000;26(1):5-16.
- Field D, Garland M, Wiliams K. Correlates of specific childhood feeding problems. Journal of Paediatrics and Child Health. 2002;39(4):299-304.
- Hofacker NV, Papousek M. Disorders of excessive crying, feeding and sleeping: The Munich interdisciplinary research and intervention program. Infant Mental Health Journal. 1998;9(2):180-201.
- Williams KE, Field DG, Seiverling L. Food refusal in children: review of the literature. Research in Developmental Disabilities. 2010;31(3):625-633.
- Mason SJ, Harris G, Blissett J. Tube feeding in infancy: Implications for the development of normal eating and drinking skills. Dysphagia. 2005;20(1):46-61.
- Byars KC, Burklow KA, Ferguson K, O'Flaherty T, Santoro K, Kaul A. A multicomponent behavioral program for oral aversion in children dependent on gastrostomy feedings. Journal of Pediatric Gastroenterology and Nutrition. 2003;37(4):473-480.
- Kindermann A, Kneepkens CM, Stok A, van Dijk EM, Engels M, Douwes AC. Discontinuation of tube feeding in young children by hunger provocation. Journal of Pediatric Gastroenterology and Nutrition. 2008;47(1):87-91.
- Garro A, Thurman SK. Kerwin ML E, Ducette JP. Parent/caregiver stress during pediatric hospitalization for chronic feeding problems. Journal of Pediatric Nursing. 2005;20(4):268-275.
- Greer AJ, Gulotta CS, Masler EA, Laud RB. Caregiver stress and outcomes of children with pediatric feeding disorders treated in an intensive interdisciplinary program. Journal of Pediatric Psychology. 2008;33(6):612-620.
- Al-Yaarubi S, Ramsay M, Rodd C. Megesterol acetate promotes euglycemia and appetite in a child with persistent hyperinsulimenic hypoglycemia. Acta Paediatrica. 2004;93(4):422-423.
- Blissett J, Harris G, Kirk J. Effect of growth hormone therapy on feeding problems and food intake in children with growth disorders. Acta Paediatrica. 2000;89(6):644-649.
- Homnick DN, Homnick BD, Reeves R, Marks JH, Pimentel RS, Bonnema SK. Cyproheptadine is an effective appetite stimulant in cystic fibrosis. Pediatric Pulmonology. 2004;38(2):129-134.
- Archer LA. Rosenblaum PL, Streiner DL. The children’s eating behaviour inventory: Reliability and validity results. Journal of Pediatric Psychology. 1991;16(5):629-670.
- Crist W, Napier-Phillips. Mealtime behaviours of young children: A comparison of normative and clinical data. Journal of Developmental and Behavioral Pediatrics. 2001;22(5):279-286.
- Wardle J. Guthrie C, Sanderson S, Rapoport L. Development of the Children’s Eating Behaviour Questionnaire. Journal of Child Psychology and Psychiatry. 2001;42(7):963-970.
- Ramsay M, Martel C, Porporino M, Zygmuntowicz, C. The Montreal Children’s Hospital Feeding Scale: A brief bilingual screening tool for identifying feeding problems. Paediatrics and Child Health. 2011;16(3):147-151.
- Dijk Maijn van, Timmerman MF, Martel C, Ramsay M: Towards the development of a Duch screening instrument for the detection of feeding problems in young children. Netherland Journal of Psychology. 2011;66(4):112-119.
- Benjasuwatep B, Rattanamongkolgul S, Ramsay M. The Thai version of the Montreal Children's Hospital Feeding Scale (MCH-FS): psychometric properties. Journal of the Medical Association of Thailand. 2015;(2)98:163-169.
- Diniz B P, Fagondes S C, Ramsay M: Cross-Cultural adaptation and validation of the Montreal Children's Hospital Scale into Brazilian Portuguese. Revista Paulista de Pediatria. 2021 Feb 24;39:e2019377.
- Garcin PRC, Ramsay M, Meyer SCL et al. Validation of the feeding scale "The Montreal Children's Hospital Feeding Scale" (mch-fs) to detect eating disorders in Mexican children. Acta Pediátrica de México. 2014;45(5):443-452.
- Sforza E, Onesimo R, Triumbari EK, Leoni C, Giorgio V, Rigante D, Kuczynska EM Ramsay, M, Zampino G. Cross-cultural adaptation and validation of the Italian version of the Montreal Children's Hospital in a special needs’ population. Language and Communication Disorders. 2023;(58):1223-1231.
- Hauser, MP, Taborda, RA, Oiberman A, Ramsay M: Escala Argentina de Dificultades Alimentarias en Nino (EADAN): Propiedades Psicometrias. Evaluar. 2019;19(2):1-14.
- Babik K, Dziechciarz P, Horwath A, Ostazsewski P. The Polish version of the Montreal Children's Hospital Feeding Scale (MCH-FS): Translation, cross-cultural adaptation, and validation. Pediatria Polka. 2019:94(5):299-305.
- Lopez AC, Guimaraes C, Afonso C. Montreal Children's Hospital Feeding Scale: Translation and contribution for the validation into European Portugeses. Revista Portuguesa De Terapia Da Fala. 2015;(3):05-15.
- Casaubon Garcin P, Ramsay M, Casaubon Lemmen Meyer S, Goldbard Rochman D, Oliva Meza Hernandez O, Baptista González H, Monroy Tenia Z, Barriguete Melendez J, Valdez M. Validación de la escala de alimentación “The Montreal Children’s Hospital Feeding Scale" (mch-fs) para detectar trastornos de la alimentación en niños mexicanos. Acta Pediátrica De México. 2024;45(5):443-452.
- Dogru I, Manav G, Uymaz P. Turkish validity and reliability study of the Montreal Children's Hospital Feeding Scale. Current Pediatric Research. 2022;26(3):1289-1296.
- Zhongxia Ren, Hanglian Lan, Ignatius Man-Yau Szeto, AI Zhao. Feeding difficulty among chinese toddlers aged 1-3 years and its association with health and development. Frontiers in Pediatrics. 2021 Nov 23;9:758176.
How to cite this article:
Ramsay M. Feeding skill, Appetite and Feeding Behaviours of Infants and Young Children and Their Impact on Growth and Psychosocial Development. In: Tremblay RE, Boivin M, Peters RDeV, eds. Faith MS, topic ed. Encyclopedia on Early Childhood Development [online]. https://www.child-encyclopedia.com/child-nutrition/according-experts/feeding-skill-appetite-and-feeding-behaviours-infants-and-young. Updated: September 2025. Accessed August 9, 2026.
Text copied to the clipboard ✓